Addison’s Disease: Clinical view of adrenal insufficiency and metabolism.
Clinical overview of adrenal insufficiency with nutrition-based metabolic support.
Addison’s Disease: A Clinical and Nutritional Perspective:
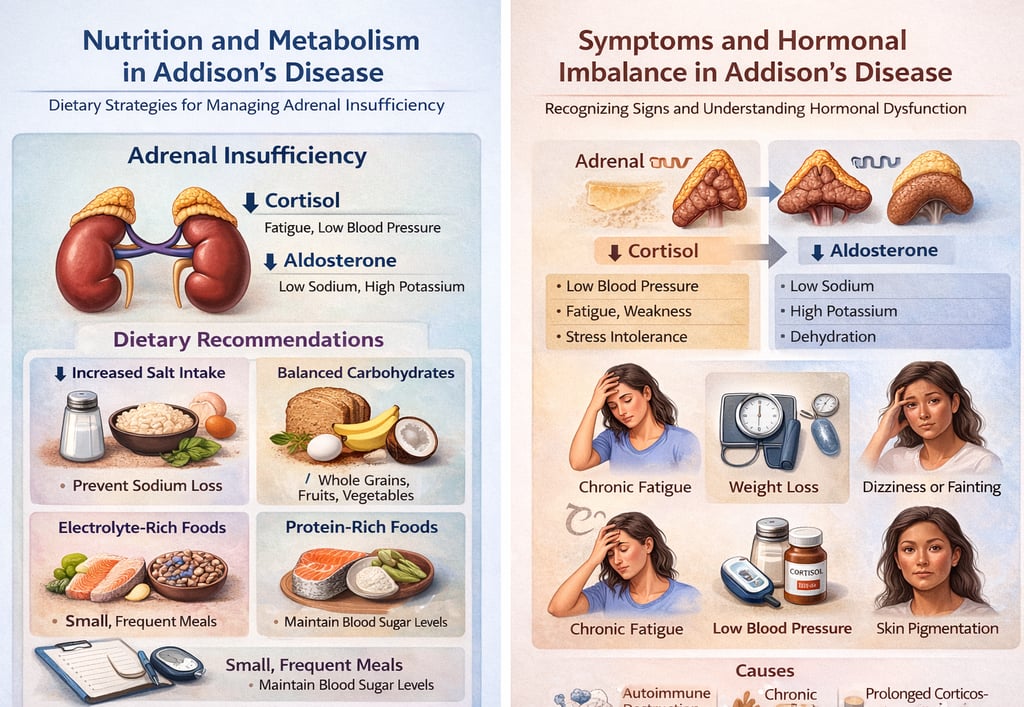
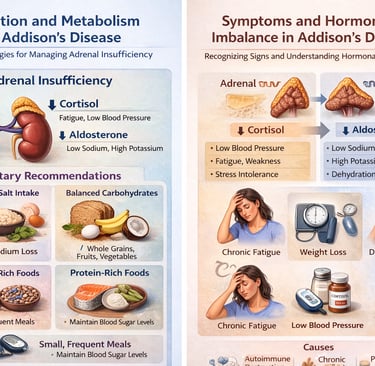
Addison’s Disease, clinically termed primary adrenal insufficiency, is an infrequent yet significant endocrine disorder characterized by the progressive or sudden failure of the adrenal cortex to synthesize adequate quantities of glucocorticoids (cortisol) and mineralocorticoids (aldosterone). These hormones are indispensable for maintaining hemodynamic stability, metabolic homeostasis, electrolyte equilibrium, and physiological stress adaptation.
Pathophysiological Mechanism
In Addison’s Disease, adrenal cortical destruction leads to:
Deficient cortisol secretion, resulting in impaired gluconeogenesis, reduced stress tolerance, and altered immune modulation
Aldosterone insufficiency, causing sodium depletion, potassium retention, and disrupted fluid balance
Progressive metabolic instability affecting multiple organ systems
The onset is often insidious, leading to delayed clinical recognition.
Clinical Manifestations
Patients may present with a spectrum of nonspecific yet progressive symptoms, including:
Persistent asthenia (fatigue) and generalized weakness
Unintentional weight reduction
Chronic hypotension with orthostatic dizziness
Electrolyte imbalance-related cravings for salt
Diffuse hyperpigmentation of skin and mucosa
Gastrointestinal disturbances such as nausea, vomiting, and abdominal discomfort
Etiological Factors
The disorder may arise due to:
Autoimmune adrenalitis (predominant etiology)
Infectious etiologies such as tuberculosis
Genetic and congenital adrenal disorders
Iatrogenic causes following prolonged corticosteroid therapy withdrawal
Rare infiltrative or hemorrhagic adrenal pathology
Nutritional Implications and Dietary Management
Nutritional therapy serves as an adjunctive supportive intervention aimed at optimizing metabolic stability and electrolyte homeostasis.
Primary Nutritional Objectives:
Maintenance of energy equilibrium
Stabilization of arterial blood pressure
Prevention of dehydration and electrolyte depletion
Restoration of sodium–potassium balance
Dietary Recommendations
1. Controlled Sodium Augmentation
Under clinical supervision, sodium intake may be moderately increased to compensate for aldosterone deficiency and prevent hyponatremia.
2. Complex Carbohydrate Optimization
Whole grains such as oats, brown rice, and millets
Provide sustained glucose release and metabolic stability
3. High Biological Value Protein Intake
Legumes, pulses, eggs, and lean animal proteins
Contribute to tissue repair and maintenance of lean body mass
4. Electrolyte-Dense Foods
Bananas (potassium regulation)
Coconut water (natural rehydration medium)
Dairy derivatives (calcium and sodium support)
5. Fractionated Meal Pattern
Frequent, small, and nutritionally balanced meals to mitigate hypoglycemia and fatigue episodes
Dietary Restrictions and Considerations
Excessive caffeine intake due to potential exacerbation of dehydration
Ultra-processed and nutrient-depleted foods
Unregulated potassium supplementation
Alcoholic beverages due to metabolic and hydration interference
Clinical Management Framework
Dietary modulation is non-curative and must be integrated with medical therapy, including:
Lifelong glucocorticoid replacement therapy
Mineralocorticoid supplementation where indicated
Periodic endocrine evaluation and biochemical monitoring
Lifestyle and Preventive Considerations
Strict adherence to hydration protocols
Avoidance of prolonged fasting states
Stress regulation strategies to minimize adrenal demand
Medical alert identification for emergency preparedness
Routine endocrinological follow-up for dose optimization
Concluding Statement
Addison’s Disease represents a chronic endocrine insufficiency disorder necessitating lifelong hormonal replacement and meticulous clinical supervision. When combined with structured nutritional intervention and lifestyle optimization, patients can achieve significant symptomatic control and improved physiological stability.